
The Holding Environment Is the First Blanket You Didn't Build
Put your hand on your ribcage. Not your chest; your ribs, on the side, just below where your arm meets your body. Breathe in. Feel the ribs expand. Breathe out. Feel them contract.
That movement is your diaphragm. A dome-shaped muscle that sits underneath your lungs and does the mechanical work of breathing. Most of the time, you don’t think about it. It contracts, your lungs fill. It relaxes, your lungs empty. Automatic. Invisible. Running in the background like everything else your body does to keep you alive.
But your diaphragm is not just a breathing muscle. It’s a regulatory organ. It sits at the intersection of two nervous system branches that determine whether you feel safe or threatened, connected or shut down, alive or numb. And the way it was calibrated; the initial settings it learned; was shaped by someone else’s diaphragm before you could hold up your own head. Every regulatory environment since then has added its own layer of training. But the diaphragm is where the story starts, and it’s where the repair starts too.
The Vagal Brake
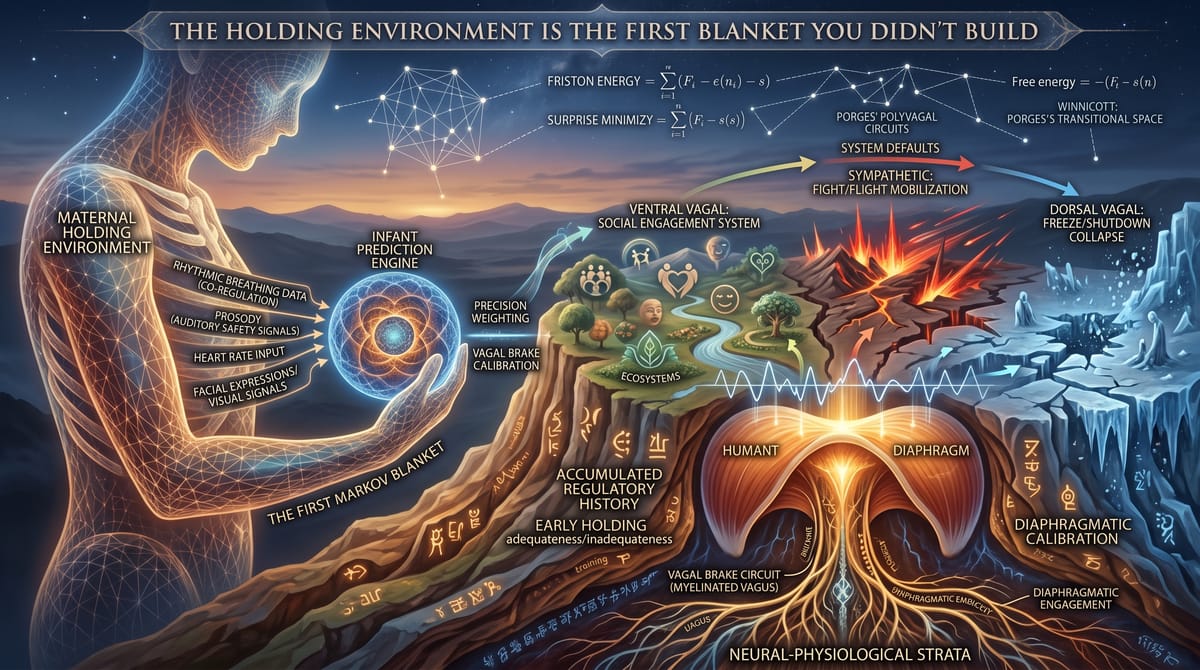
Stephen Porges, the neuroscientist who developed polyvagal theory, mapped three circuits in the autonomic nervous system. Not two, the way most people learned it. Three.
The ventral vagal circuit is the newest, evolutionarily. It governs the social engagement system; the face, the voice, the middle ear, the heart, and the breath. When this circuit is online, you feel safe. You can connect. Your face is expressive, your voice has prosody, your breathing is slow and rhythmic. You can listen, you can process nuance, you can be present with another person without mobilizing for defense.
The sympathetic circuit is older. Fight or flight. When this circuit activates, your system has determined that the environment is threatening and you need to act. Heart rate increases. Breathing gets shallow and fast. Muscles tense. Blood flow shifts to the limbs. The social engagement system goes offline because you don’t need to be charming when you’re running from a predator.
The dorsal vagal circuit is the oldest. Freeze. Shutdown. Collapse. When this circuit takes over, the system has determined that neither fight nor flight will work and the best survival strategy is to conserve energy and disappear. Heart rate drops. Breathing becomes minimal. You go numb. You dissociate. You leave the building, perceptually, even though your body is still in the chair.
Porges’ key insight is that these aren’t just reactions. They’re hierarchical. The system defaults to the most evolved circuit first. Ventral vagal: social engagement. If that fails to resolve the threat, the system drops to sympathetic: mobilization. If that fails, it drops to dorsal vagal: immobilization. The hierarchy maps the evolution of survival strategies, and it operates the same way in a therapy session as it does in a jungle.
The mechanism that keeps you in ventral vagal; the thing that prevents unnecessary drops into sympathetic activation; is called the vagal brake. It’s a regulatory function of the myelinated vagus nerve, and it operates substantially through the diaphragm. When your diaphragm is moving slowly and fully; the long, deep breathing that marks a regulated nervous system; the vagal brake is engaged. It’s holding the system in the ventral zone. Slow breath, social engagement online, prediction engine running in exploration mode rather than defense mode.
When the breath gets shallow and fast, the vagal brake releases. The system drops. And once it drops, the prediction engine shifts from modeling the world as a place to explore to modeling the world as a place to survive.
The First Breath You Didn’t Take Alone
Here’s where Winnicott and Porges converge, and the move is as precise as anything in Friston.
The infant’s vagal brake is not calibrated at birth. It can’t be. The myelinated vagus, the circuit that governs social engagement, is still developing. The baby doesn’t have the physiological architecture to regulate its own autonomic state. It can’t breathe itself calm. It can’t hold itself in ventral vagal. It doesn’t have a functioning vagal brake yet.
What it has is its mother’s.
When the mother holds the infant against her body, the infant’s nervous system isn’t just receiving warmth and pressure. It’s receiving rhythmic data. The mother’s breathing rate, transmitted through the chest wall, through the physical contact of skin and rib and muscle, becomes the infant’s sensory input for what “regulated” feels like. Her slow, deep breaths move the infant’s body. Her diaphragm teaches the infant’s diaphragm the rhythm. Her vagal brake, operating through her own myelinated vagus, functionally extends to the infant’s system through the coupling of their bodies.
Her prosody does the same work through a different channel. The sing-song voice that adults instinctively use with babies isn’t arbitrary. It’s a specific frequency range that the infant’s middle ear is calibrated to receive. It signals ventral vagal safety through the auditory system. The pitch, the rhythm, the rising and falling tones; these are sensory inputs that tell the infant’s prediction engine: the environment is safe. Stay ventral. Don’t drop.
Her heart rate, transmitted through contact. Her facial expressions, processed through the infant’s still-developing but already active visual system. Her smell, her microbiome, the biological signals that pass between bodies in close contact. All of it, all of it, is the holding environment doing its regulatory work. The mother’s ventral vagal state is the first Markov blanket the infant experiences. Her nervous system is the boundary between the baby and chaos.
The clinical utility of this model is enormous, even where the evolutionary neuroscience remains contested. (Porges’ specific claims about the phylogenetic hierarchy of vagal circuits have drawn pushback from some evolutionary biologists; the three-circuit architecture is a useful clinical map, not settled anatomical fact, and this book treats it as such.) What is well-established is the broader point: the infant’s autonomic regulation is substantially outsourced to the caregiver’s body. The good-enough mother isn’t just emotionally responsive; she’s autonomically present. Her regulated state co-regulates the infant’s state through measurable, physical channels. Her diaphragm teaches the infant’s diaphragm. Her vagal brake functionally extends to the infant’s heart.
When Winnicott said the holding environment, he meant a body holding a body, a nervous system holding a nervous system, a regulated system wrapping around an unregulated one and providing the conditions for regulation to develop. Porges gave this the neuroscience. Friston gave it the math. The prediction engine’s initial calibration; its first parameters for whether the world is safe or threatening; was set by someone else’s breath.
But the calibration didn’t end there, and this matters. Every close physical relationship you’ve had since has layered its own training onto the vagal system. The friend whose presence always settled you taught your nervous system something. The partner whose dysregulation kept pulling you out of ventral taught it something else. The years you spent in high-stress work environments, breathing shallowly for eight hours a day, trained the diaphragm into patterns the holding environment never installed. The initial parameters matter; they set the architecture. But the architecture has been modified by every regulatory environment since. You’re not running infant software on adult hardware. You’re running a system that has been trained by every body that ever held yours, and by every environment that taught your diaphragm what “normal” breathing looks like.
What the Holding Environment Teaches the Prediction Engine
The three-tradition synthesis lands here.
Winnicott: The holding environment is the relational space where the infant learns to tolerate prediction error. A good-enough mother provides consistent-but-imperfect care, which means the infant experiences the gap between expectation and reality in doses it can metabolize. This builds the architecture for flexible model updating.
Porges: The holding environment is the autonomic training ground where the infant’s vagal brake gets calibrated. The caregiver’s regulated nervous system provides the co-regulatory input that teaches the infant’s system what ventral vagal safety feels like, how to return to it after activation, and how much prediction error can be tolerated before the system needs to drop into defense.
Friston: The holding environment is the first external system that shapes the infant’s precision weighting. The caregiver’s patterns of response; which signals she responds to, how quickly, how accurately; teach the infant’s prediction engine how much weight to assign to different classes of sensory input. Distress signals get high precision because the mother responds to them. Mild discomfort gets lower precision because the mother lets the infant sit with it for a moment before intervening. The entire architecture of precision weighting; the architecture that will later determine whether this person is securely attached, anxiously attached, or avoidant; is being configured by the caregiver’s response patterns, transmitted through the body, processed by a prediction engine that doesn’t yet know it exists.
Three frameworks. One mechanism. The mother’s nervous system, in physical contact with the infant’s nervous system, calibrating the prediction engine that will run for a lifetime.
What This Means for Your Diaphragm Right Now
If you’ve ever been told to “take a deep breath” when you’re upset, you’ve been given correct advice with no explanation of why it works. Here’s why it works.
When you breathe diaphragmatically; slow, deep belly breaths rather than shallow chest breaths; you’re engaging the vagal brake. The physical action of the diaphragm moving fully through its range stimulates the myelinated vagus nerve. This shifts the autonomic system toward ventral vagal. Heart rate slows. The social engagement system comes back online. The prediction engine, which had been running threat models, starts running connection models again.
But here’s the deeper frame. When you breathe diaphragmatically, you’re not just calming down. You’re reactivating a co-regulatory circuit that was supposed to be calibrated by another nervous system when you were too young to remember. You’re doing for yourself, consciously, what a good-enough mother’s body did for you automatically. The slow, full movement of the diaphragm is the adult version of being held against a regulated chest.
For people whose accumulated regulatory history is mostly positive; good-enough early holding, relationships that provided co-regulation, environments where the vagal brake got regular exercise; this comes relatively naturally. The system knows what regulated feels like and can find its way back. Diaphragmatic breathing is a reinforcement of existing architecture.
For people whose regulatory history has been rougher; early holding that was inadequate, relationships that kept the system in chronic activation, work environments that trained shallow breathing as the default; the vagal brake may never have been properly calibrated, or it was calibrated and then de-calibrated by years of conditions that didn’t support it. Diaphragmatic breathing is harder for these people, not because they lack discipline, but because they’re working against accumulated training. The circuit was either never completed or was overwritten by subsequent environments that rewarded activation over regulation.
This is why breathing exercises feel different for different people. It’s not willpower. It’s not practice alone. It’s the accumulated state of the co-regulatory circuit across your entire regulatory history. And knowing this changes the practice from a wellness technique to a developmental intervention. You’re not managing stress. You’re retraining a circuit that was shaped by every environment your body has lived in.
The Practice
Here’s what you can do with this, starting now.
Sit somewhere quiet. Put one hand on your belly, below your navel. Put the other on your ribs, on the side. Breathe in through your nose, slowly, and direct the breath downward. Feel your belly push out against your hand first, then feel your ribs expand laterally. Hold for a beat. Not a long hold; just a pause at the top. Then exhale slowly through your mouth, longer than the inhale. Feel the ribs come in. Feel the belly flatten.
That’s diaphragmatic breathing. The ratio matters: the exhale should be longer than the inhale. A four-count inhale and a six-count exhale is a good starting point. The extended exhale is what engages the vagal brake. It’s the physiological signal that tells the autonomic system: we’re not in danger. We can afford to slow down.
Do this for two minutes. That’s enough to shift the autonomic state measurably. Not conceptually; measurably. Heart rate variability changes. Cortisol begins to drop. The social engagement system starts to come back online.
Now here’s the deeper practice. While you’re breathing, notice what happens in your prediction engine. Notice the thoughts that arise. Notice whether your system wants to speed up, to check your phone, to plan something, to worry about something. Those impulses are your prediction engine generating models of the world that require action. The sympathetic system wants to mobilize. The dorsal system wants to disappear. The vagal brake, engaged through the breath, is holding you in the space where neither defense is necessary.
This is the holding environment, rebuilt from inside. Your diaphragm, doing the work that every previous regulatory environment either completed or didn’t. Your vagal brake, engaging a circuit that was shaped by someone’s arms, then by every relational and physical environment since. Developmental repair, two minutes at a time, through the one muscle that connects breath to safety to the prediction engine’s capacity to tolerate being alive in a world that doesn’t always match what you expected.
The holding environment is the first Markov blanket you didn’t build yourself. Every relationship since has modified the blanket in ways you may not have chosen. This practice is how you start building your own.